Antenatal Cardiology
Semilunar = Aortic and Pulm
AV = Tricusp and Mitral (the only bicusp)
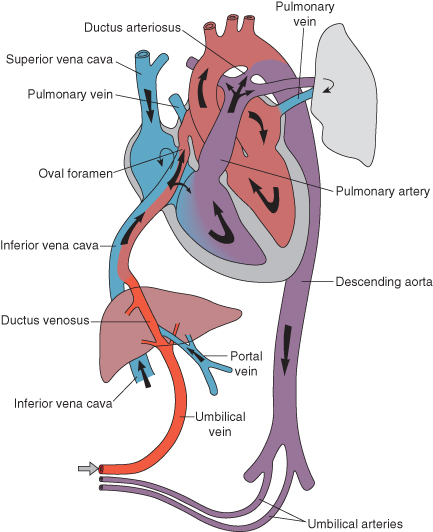
R>L shunt across PFO and PDA
High Pulm Vasc Res
Low Pulm flow
Pulm vasc resistance falls, R>L PFO shunt ceases
Ductus arteriosus closes
Ductus venosus closes
Dilatation from regurgitation is the main cause of fetal comprimise. Most other lesions are tolerated until birth
Heart failure leads to Fetal Hydrops (accumulation of pericardia/pleural/peritineal/subcutaneous fluid)
OR Fetal loss
<24hr
Respiratory distress > CXR ?cardiomeg ?pulm vasc
Murmur
Cynosis
------------
24hr to 2w
Dependent on PDA for pulm
Dependent on PDA for systemic flow
PDA dependent for mixing > Cyanosis
Hyperoxia test
If Cyanotic > CXR
Boot shape TOF
TAPVD: R> L PFO to compensate
--------------------
2-6w
Pulmonary vascular resistance falls > congestive cardiac failure
tachypnea
poor feeding
poor weight gain
hepatomegaly
sweaty
tachycardic
VSD w Coarct
PDA, large VSD, CAVC
Truncus (PArt comes of truncal vessel),
TOF w PA: with Major Aortopulonary Collaterals (MAPCs) essentially pulm arteries of aorta
sing vent no PS
--------------------
Asymptomatic murmurs
50% of kids will have a murmur at some stage
15% have grade 2 or more
Most don't have disease and don't require further investigation
Ask about exercise intolerance, recurrent respiratory infections
Functional commonest
ASD - hyperdynamic precordium (visibly moves to much), wide fixed S2, systolic flow (of extra left fluid going through TV)
VSD
PS, AS, (ejection click from stiff leaflets)
Cooarct, PDA...
triggers for Ix
murmur loud
loud S2
abnormal pulses
Failure
Delay between 18mo and 3yo if well as ECHO difficult and no damage from delayed diagnosis
Coarct: posterior (between scapula) murmur, fem pulses down, hypertension,
Still's murmur: well, no failure, normal precordium, softer on sitting, louder with fever, normal S2, twang of string
Venous hum: reduces on turning head occluding vein
PATHOLOGIC murmurs are never intermittent
Refer: abnormality found HxEx, young, anxious
AV = Tricusp and Mitral (the only bicusp)
R>L shunt across PFO and PDA
High Pulm Vasc Res
Low Pulm flow
Pulm vasc resistance falls, R>L PFO shunt ceases
Ductus arteriosus closes
Ductus venosus closes
Dilatation from regurgitation is the main cause of fetal comprimise. Most other lesions are tolerated until birth
- TR, Epsteins anomaly (low tricusp leaflets > large RA small RV
- CAVC (Complete Atrioventricular Canal Defect)
- Truncus
- Complete Heart Block
- Atrial arythmias
Heart failure leads to Fetal Hydrops (accumulation of pericardia/pleural/peritineal/subcutaneous fluid)
OR Fetal loss
<24hr
- Valve regurg: Epsteins (huge heart), absent pulm valve syndrome (resp distress as big arteries press of bronchioles)
- Obstructed TAPVD (pulm congestion on CXR, confused with PPHN, not being uniform is suggestive of TAPVD/pneumonia)
- Early duct dependent lesion
Respiratory distress > CXR ?cardiomeg ?pulm vasc
Murmur
- in in first 24 hours is before Pulm vas drop = semilunar valve (AS/PS) stenosis, AV valve (MS/TS) stenosis
- AVD/VSD don't declare until pulm vessels fully relax after 24 hours
Cynosis
- <24h ?mixing e.g. TGA, Single vent
------------
24hr to 2w
Dependent on PDA for pulm
- severe cyanosis e.g. critical PS, Pulm atresia, either with single vent
Dependent on PDA for systemic flow
- Shock e.g. critical AS, critical coarct, HLHS (hypoplastic left heart i.e. under-developed)
PDA dependent for mixing > Cyanosis
- TGA - narrow mediastinum, plethoric lungs needs ballon atria septostomy
Hyperoxia test
If Cyanotic > CXR
- Massive cardiomegaly - Epsteins
- Congestion or figure 8 / snowman - TAPVD
- Plethoric (prominent vessels) or Egg on string (great vessels end up in line AP) - TGA
- Oligemic (reduced blood flow) lung fields - PS/PA
Boot shape TOF
TAPVD: R> L PFO to compensate
--------------------
2-6w
Pulmonary vascular resistance falls > congestive cardiac failure
tachypnea
poor feeding
poor weight gain
hepatomegaly
sweaty
tachycardic
VSD w Coarct
PDA, large VSD, CAVC
Truncus (PArt comes of truncal vessel),
TOF w PA: with Major Aortopulonary Collaterals (MAPCs) essentially pulm arteries of aorta
sing vent no PS
--------------------
Asymptomatic murmurs
50% of kids will have a murmur at some stage
15% have grade 2 or more
Most don't have disease and don't require further investigation
Ask about exercise intolerance, recurrent respiratory infections
Functional commonest
ASD - hyperdynamic precordium (visibly moves to much), wide fixed S2, systolic flow (of extra left fluid going through TV)
- secundum
- venous
- Primum - can effect MV
VSD
PS, AS, (ejection click from stiff leaflets)
Cooarct, PDA...
triggers for Ix
murmur loud
loud S2
abnormal pulses
Failure
Delay between 18mo and 3yo if well as ECHO difficult and no damage from delayed diagnosis
Coarct: posterior (between scapula) murmur, fem pulses down, hypertension,
Still's murmur: well, no failure, normal precordium, softer on sitting, louder with fever, normal S2, twang of string
Venous hum: reduces on turning head occluding vein
PATHOLOGIC murmurs are never intermittent
Refer: abnormality found HxEx, young, anxious