Bronchiectasis
Epidemiology
Pathophysiology
Hx
DDx
Ix
Complications
- CF 1:2500 in Oz
- Non CF Bronchiectasis in remote indigenous 15:1000!
Pathophysiology
- variable leading to bronchial walls that are weak, dilated, collapsible, chronically inflamed, and plugged with mucus secretion
- chronic obstructive lung disease
- Leads to atelectasis, emphysema, fibrosis, and hypertrophy of the bronchial vasculature
- Common pathogens (Streptococcus pneumoniae, Haemophilus influenzae, and Moraxella catarrhalis)
- Can achieve reversal of disease in postinfection / treated primary immunodeficiency
Hx
- Chronic productive cough
- purulent sputum common (not seen as swallowed in young)
- Haemoptysis uncommon (from eroded blood vessels)
- Recurrent exacerbations with fever and increased productive cough, pleuritic chest pain, dyspnoea
- Dyspnoea
- Exercise intolerance
- Steatorrhea (CF)
- Choking (FB
- Dysmorphology (VACTERL > TOF, any of CHD)
- FTT (CF, Immunodeficiency)
- Clubbing
- Cyanosis
- Sinusitis (CF, immunodeficiency, PCD)
- Chronic OM (PCD)
- Scoliosis
- Crackles, rhonchi (coarse expiratory breath sound), wheeze
- Hyperinflation: barrel chest
- Dextrocardia (Kartagener)
- Neurological Ex
DDx
- Congenital (tracheobronchomalacia)
- Bronchial obstruction
- Congenital (CCAM, pulm sequest)
- FB
- mucous impaction (asthma, ABPA) hilar adenopathy (TB) tumour
- Immunodeficiencies (SCID, C3C4 def, HIV)
- Secretion clearance (CF, PCD/Kartagener)
- Neurological (poor cough in NM)
- Infection (staph, pseudom, adeno, TB, recur asp)
- Environmental (talc, smoke)
- Autoimmune (scleroderm)
- Genetic (Yellow nail syndrome, A1AT deficiency)
Ix
- CXR
- Linear atelectasis, Tram-tracking, ring shadows
- Upper ?CF/TB/aspiration in nonambulant
- Middle: ?PCD
- Central airways ?ABPA ? Asthma
- Lower: immunodeficiency, sequestration, aspiration in ambulant
- Pulmonary vascular hypertrophy
- Linear atelectasis, Tram-tracking, ring shadows
- HR CT if CXR not diagnostic
- "signet ring" shadows (airway > artery within 2cm of pleura)
- Sweat test
- Nasal brushings (or bronchial) for high speed video microscopy and TEM
- IgE: total and Aspergillus fumigatus (ABPA)
- Quantiferon gold
- Immune function
- FBE
- Ig levels
- Vaccine responses ie Humoral panel (antitetanus, antidiphtheria, and antipneumococcal antibodies)
- HTLV1 in indigenous
- Bronchoscopy and BAL
- PFTs (can have obstructive and restrictive)
- Antibiotics (can be reversible if chronic infection is the primary cause)
- Rx underlying cause (FB, immunodeficiency, aspiration)
- Promote lung health
- Nutrition
- Immunisation
- Avoid infection (hygiene), environmental (smoke/fire), allergens
- Prevent progression
- Improve mucocilary clearance
- Physiotherapy (postural drainage and percussion , breathing and coughing exercises, Vest)
- NOT Pulmozyme (used in CF but potentially harmful in nonCF)
- Bronchiodilators if PFTs show response
- Rx infective exacerbations
- target previous organisms > Cipro for pseudomonas
- Inhaled tobramycin month on month of for chronic pseudomonas
- Empirical in absence of organisms > Augmentin or Azythromycin for 14days
- target previous organisms > Cipro for pseudomonas
- Improve mucocilary clearance
- Control inflammation
- Azythromycin for combined antiinflammatory / antibiotic properties
- Supplemental O2 if hypoxaemic
- Embolisation / surg for massive haemoptysis
- Lobectomy if localised with severe symptoms (FTT, recurrent infections, massive haemoptysis)
- Transplant
- Surveillance of complications
Complications
- Hypoxia > Pulmonary hypertension > cor pulmonale
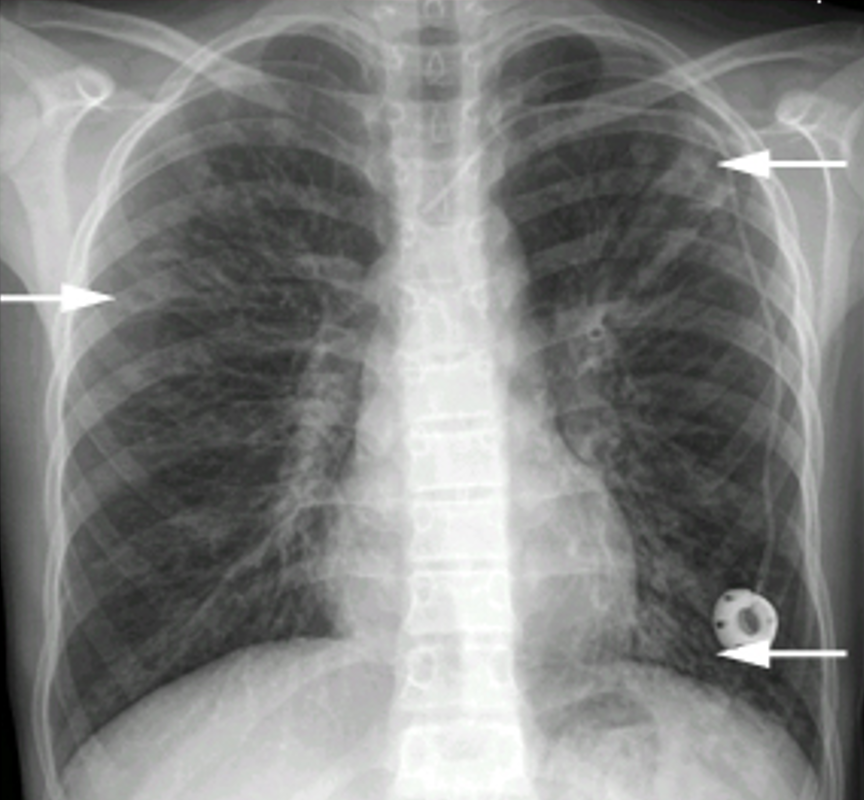
Lower arrow: tram tracking
Upper arrows: ring shadows