Graft Versus Host Disease
engraftment of immunocompetent donor lymphocytes in an immunologically compromised host that shows histocompatibility differences with the donor
donor T-cell activation against recipient major histocompatibility complex (MHC) antigens or minor histocompatibility antigens
Acute (within 3m)
Chronic (more resembling systemic rheumatological disease e.g. SLE)
Acute
Pathophysiology
Ix
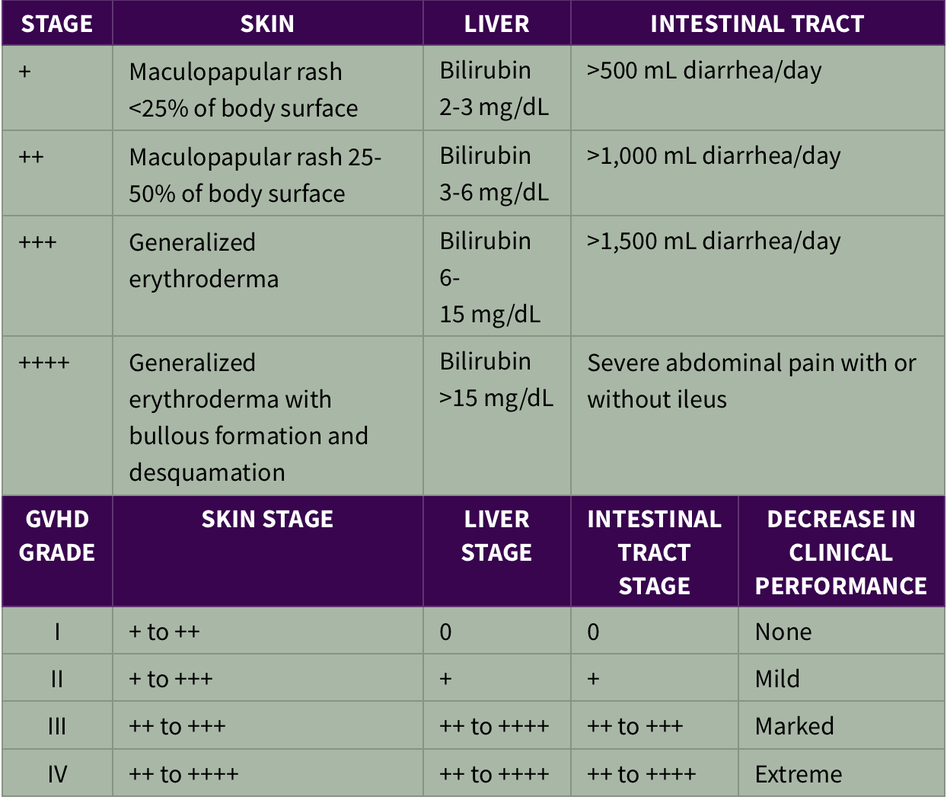
Grade I: skin only
Grade 2: moderate
Grade 3: severe
Grade 4: life threatening
Prevention:
Rx with glucocorticoids
for steroid resistant: Antithymocyte globulin, mycophenolate mofetil, pentostatin, extracorporeal photopheresis, or monoclonal antibodies all tried. No superior Rx established
donor T-cell activation against recipient major histocompatibility complex (MHC) antigens or minor histocompatibility antigens
Acute (within 3m)
Chronic (more resembling systemic rheumatological disease e.g. SLE)
Acute
Pathophysiology
- Tissue damage in host leads to APC presenting self to donor T-cells
- donor T cells activat, proliferate, expand, and generate cytokines: TNF-α, IL-2), IFN-γ
- These cytokines cause tissue damage and promote differentiation of cytotoxic CD8+ T cells, which together with macrophages kill recipient cells
- 2-5w post transplant
- erythematous maculopapular rash
- persistent anorexia, vomiting and/or diarrhea
- liver disease
Ix
- skin, liver, or endoscopic biopsy for confirmation
Grade I: skin only
Grade 2: moderate
Grade 3: severe
Grade 4: life threatening
Prevention:
- immunosuppression e.g. cyclosporine or tacrolimus in combination with methotrexate or prednisone or others
- T-cell depletion of graft
Rx with glucocorticoids
for steroid resistant: Antithymocyte globulin, mycophenolate mofetil, pentostatin, extracorporeal photopheresis, or monoclonal antibodies all tried. No superior Rx established
Chronic GVHD
Acute is the greatest risk for chronic
Acute is the greatest risk for chronic