Neurology Ex
Short cases
Neurological Dx
Upper (inc developmental) v Lower v Muscle
(sticker on stop watch)
I have Washed my hands
Introduce
Stand back
Exposure: at least in shorts
Position: Standing then sitting then lying then gait
Order: Cortical > CN > Trunk > Limbs
Inspection
Equipment
Dysmorphism (unusual morphological features)
Observations
Growth
Protein adipose
Play ball with preschoolers to improve rapport / get initial impression
Observe with a toy/drawing/play with ball
Shake hands with child and parents
Myotonia: difficulty relaxing contracted muscle (myotonic dystrophy)
Anthopometry
- Microcephaly
- Macrocephaly
General Appearance
- AVPU
- Crutches, splints, orthoses, wheelchair, inspect shoes (symmetry > hemiplegia, symetrical > diplegia)
- Dysmorphology
- T21 (ears, eyes)
- Short neck (Klippel-Feil)
- Neurocutaneous stigmata
- Sturge-Weber (facial angioma)
- TSC (Ash leaf
- NF1 (Cafe-au-lait, axillary freckling, neurofibromas)
- ?hair loss ? seen in LMN
- Scars (muscle biopsy, tendon release)
- Eyes: strabismus, ophthalmoplegia
- Face: Myopathic facies (NMJ ie MG, Myopathies) Bell's Palsy (CN VII/UMN)
Fasciculations (LMN)
---------
Posture
- Eye deviate away from irritation seizure / towards destruction
- Hemi/Di/Quadraplegic
- Dystonic: unusual posturing (basal nuclei), opisthotonus (back arched, ExPyr)
- Hypotonic (hypotonic weak = LMN, hypotonic not weak = UMN)
- Frog-legged = LMN
- Brachial plexus
- Upper - Erb's: Waiters tip (C5,6)
- Lower - Klumpke's: Claw hand (all digits) (C8,T1)
- Radial nerve palsy: wrist drop
- Medial nerve: monkey hand
- Ulna nerve: ulna claw (4th and 5th digits)
Back
- Shunt/cochlear
- Neck
- Scoliosis (UMN/LMN/myopathy)
- Name by direction of convexity ie direction of movement
- Cobb angle (intersection of lines through lower margin of upper and lower most angulated vertebral bodies) >10 significant
- Hairy patch
- Meningomyelocele
- Touch the toes and check the spine
Movements
- Handedness
- Chorea: quick, distal muscles (UMN ?CP)
- Athetosis: slow, writhing (UMN ?CP)
- Ballismus: quick proximal
- Myoclonus: quick jerk of a muscle or group
- Tremor: rhythmic
- during writing: ?essential ?familial
- intention aka cerebellar: finger nose > slow rhythmic perpendicular movements with dysmetria aka past pointing
- Tic: repetitive stereotyped (Tourette)
Cranial bruit
------------
Cortical/development
- MMSE
- Development: give toys
- Attention, fine motor, visual-spacial abilities
- dysphasia: Wernicke's (temporal usually L hemisphere) problem of language
- dysarthria: Broca's (frontal usually in L or CNVII,VIII,IX,X,XII or cleft) problem of speech
Galant reflex: paraspinal stimulation causes reflex flexion
Sphincter tone (frontal)
Personality (frontal-irritable/lethargic,temporal-psychotic aggressive)
Spatial perception (non-dominant temporal)
Number recall (temporal)
Apraxia - series of tasks (parietal)
Parietal Dominant
- Wernicke's: receptive dysphasia
- Broca's: expressive dysphasia
--------------
Cranial nerves
CN 0 – Terminal: variable presence, vestigial ?pheromone sensor
CN I – Olfactory
- blow nose - chocolate
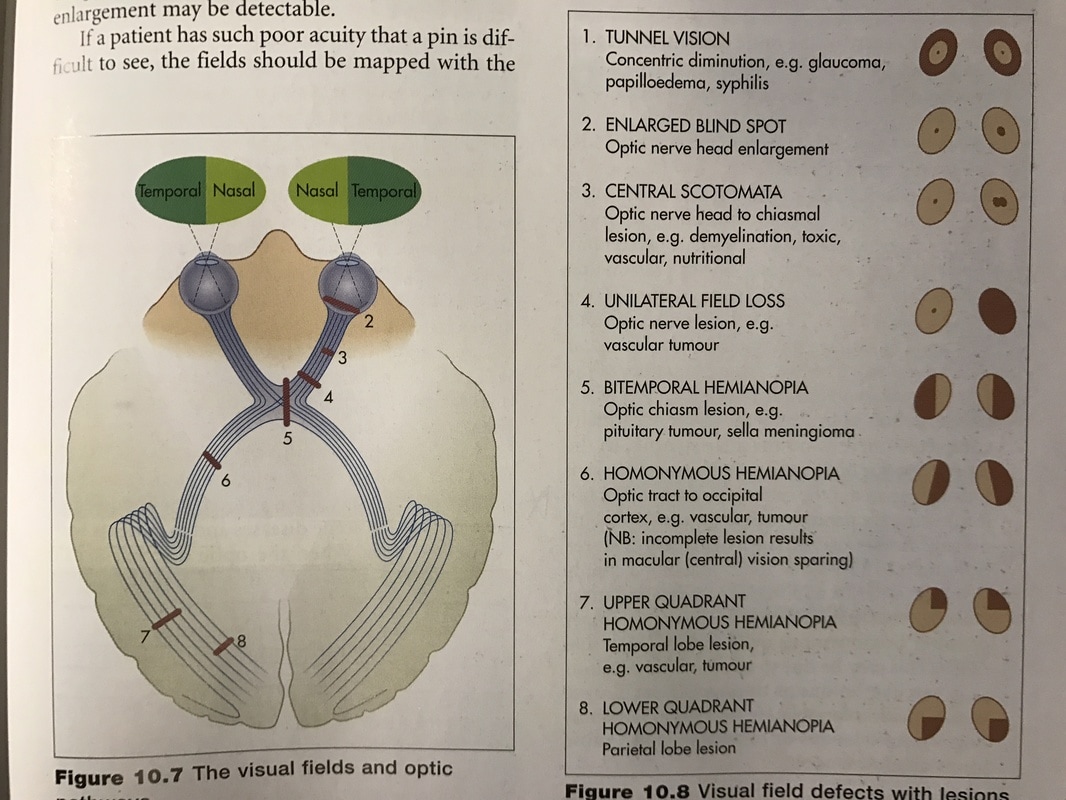
- VF distract then red toy from behind for fields (below)
- Tunnel vision: Glaucoma, papilloedema
- Macular degeneration
- unilateral (full) field: ipsilateral (optic) nerve
- bitemporal hemianopia: Chiasmal
- homonymus: contralateral tract
- VA - Cover and offer and object, Striped cloth, E, object, Snellen
- Fundoscopy - tell me when mum sticks her tongue out
CN III – Oculomotor
- ptosis
- eye down and out
- dilated (mydriasis) unresponsive pupil (contralateral constriction to light intact) (v Horner's with ptosis and small pupil)
- Eye up and in
- sup oblique intorts
- Masseter bite (bottle/lolly) (eff)
- Pterygoids: open mouth (deviates to weak), push against hand with jaw
- sensation (aff) (Ophth, Max, Mand),
- Jaw jerk (both) up in pseudo bulbar palsy
- corneal (V/VII)
- Eye in or slight head tilt towards affected side to make congruent
- Lat rectus (i.e. diplopia worse left and left image disappears on closing = L CNVI)
- Dolls eye reflex neonate/coma/obscured fixation
- Bell's palsy (80%) if LMN check for ear/palate erythema/vesicles ?Ramsay-Hunt
- Muscles of facial expression
- Look up (spared in UMN)
- Shut eyes tight
- Nasolabial fold
- Show teeth
- Blow cheeks out
- stapedius muscle
- taste in anterior ⅔ of tongue (ant to ear)
- Look for vesicles
- Feel for cochlear implant
- 68 high freq
- 100 low freq
- if problem then check (DDx neurocuteneous, Alports if bilateral)
- Rinne (256) mastoid until sound gone, then external meatus, normal is can hear again (i.e. air conduction better then bone)
- Weber: centre of head (louder in affected ear if conduction, louder in unaffected if sensorineural)
- sensation posterior pharynx L+R (taste posterior ⅓ of tongue not routinely tested, post to ear)
- (gag tests IX/X together if can't cooperate)
- 'Ah' uvula deviates towards normal side (away from lesion)
- Swallow water (look for cough/nose regurg)
- speak and cough: hoarse voice / bovine cough = recurrent laryngeal nerve lesion (branch of vagus)
- (gag tests IX/X together if can't cooperate, need to do both side to see if palsy)
- Shrug shoulders against resistance note Trap bulk
- Turn head against resistance note SCM bulk (R turns L and vv)
- Wasting vesiculations of tongue (LMN)
- tongue straight, left and right, deviates to side of lesion (LMN as bilateral UMN innervation)
Parinaud's syndrome
Strabismus
- Congenital limitation in medial or lateral gaze ?Duane syndrome
Acute Peripheral facial neuropathy (VZV V: HZ Ophthalmicus, VZV VII/VIII: Ramsay Hunt)
(Moebius syndrome = VI/VII palsy)
Bulbar palsy = LMN 9,10,12 (pseudo is UMN) (bulb = bottom of brain stem)
Horners: ptosis, miosis, and anhidrosis SNS ?Neuroblastoma (listen to chest) birth trauma ? Klumpke (look at neck)
Ix MRI head and neck
CT neck and chest if horner
---------
Limbs (motor unit = 1 lower motor neuron + the muscle fibres it innervates)
Upper limb
Posture
Wasting, fasciculation (LMN)
Scars (tendon release, biopsy)
Compare nail beds (asymmetric growth arrest)
Pronator drift (proprioception loss (posterior column), cerebellar hypotonia or pyramidal weakness)
Palpation
- feel muscle bulk
- Muscle tenderness (dermatomyositis)
- Ulna nerve hypertrophy at elbow (Charcot-Marie-Tooth / Leprosy)
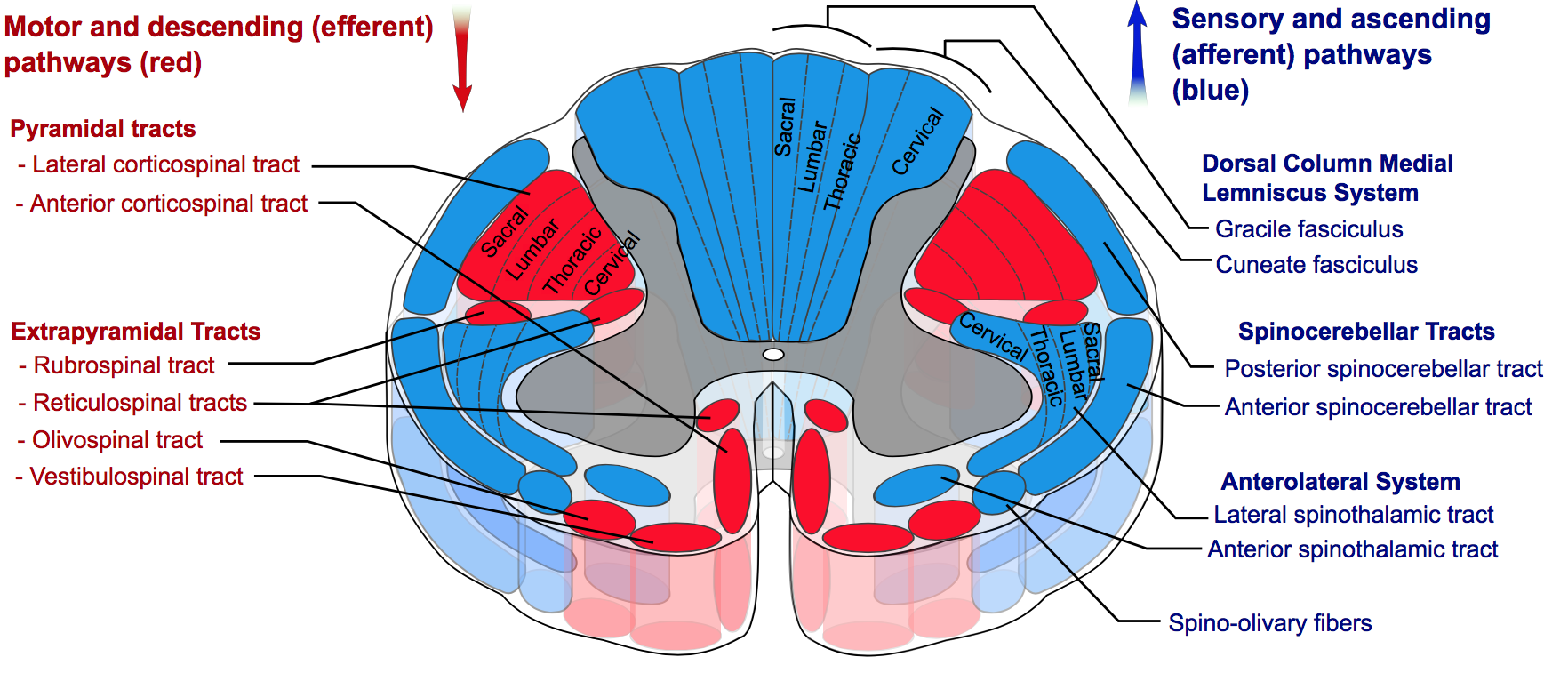
- Increased (UMN)
- Spasticity (increased in one direction, worse with speed) (Pyramidal: eg corticospinal)
- Clasp-knife: initially high then givesway
- Rigidity (same in both directions and independent of speed) (Extrapyramidal: rubrospinal/vestibulospinal)
- Leadpipe: persistant
- Cogwheel: persistent with intermittent worsening (overlying tremor)
- Paratonia (anxiety related need to overcome with distraction)
- Spasticity (increased in one direction, worse with speed) (Pyramidal: eg corticospinal)
- Decreased (LMN)
Power - proximal: myopathy, distal: neuropathy except Myotonic Dystrophy (distal weakness, myotonia)
- Shoulder aBd (C4/5), aDd (C6/7/8)
- Elbow Flex (C5/6), Ext (C7/8)
- Wrist flex/ext (C6/7)
- Finger flex/abd (C8/T1)
- Thumb ext (Radial)
- Thumb aBd then 'ok'sign (2 branches of median)
- Little (or all finger aBd) (Ulnar)
Power (weakness)
- 0: nil
- 1: flicker, no movement
- 2: movement without gravity, no antigravity
- 3: antigravity, no resistance
- 4: reduced resistance
- 5: normal resistance
Distal: grip/wrists/ankles (foot drop, heal walking, toe walking) ?neuropathy
Reflexes with reinforcement (up in UMN)
- BJ/BRJ (C5/6)
- TJ (C7/8)
- Proprioception (posterior column)
- Distal phalanx from sides after demonstration with eyes open
- Rhombergs
- Vibration (posterior column) 'tell me when the boxing has stopped'
- Spinothalamic
- Light touch (cotton wool)
- Pain: sharp or dull
- (temperature)
- Laterally: shoulder (C4), arm (C5, forearm (C6). Finger tips (C7). Medially forearm (C8), elbow (T1), axilla (T2).
- Dorsum of distal IP of thumb (radial), middle (median), and little (ulna)
- Finger nose for intention tremor, jerky (dysynergia), past pointing (dysmetria) (cerebellum)
- pen in lid as alternate for younger
- Dysdiadochokinesis: pronate/supinate
- Mime ADLs with pens: brush hair, brush teeth, cut steak, sign the bill, drink to celebrate
Lower Limb
Pants and shoes (inspect) off
Inspection
As above including Back
Calf hypertrophy (Duchenne's)
Pes cavus (neuromuscular disease)
Palpation of muscle bulk, tenderness (dermatomyo), hypertrophied lateral popliteal nerve
Tone inc clonus at knee (push patella inf) and ankle (10 normal in <2mo)
Power
Knee to chest: Hip Flexion (L1/2/3)
Kick me away: Knee Ext (L3/4)
Toes up: Dorsiflexion (L4/5)
Knee into bed: Hip ext (L5/S1/S2)
Foot bum: Knee flex (L5/S1)
Toes down: Plantar flex (S1)
Reflexes with reinforcement
KJ L3/4 (Crossed adductor or spreading = UML)
AJ S1/2
Plantar reflexes:
- Chaddock > stroke lateral side of foot. up after 18mo = UMN
- Gonda > flick fourth toe
- Babinski's ie sharp object to sole more likely to give withdrawal in children
Coordination
heal shin
toe-finger
tap foot on hand
Sensation
L1 Groin
L2 ant thigh
L3 knee
L4 medial leg
L5 lateral leg
S1 lateral foot
S2 posterior thigh
Gait (thighs, knee, ankle, foot)
- Toe walking
- Heal walking (if can't ?peroneal weakness ?contracture)
- Heal-toe walking (achieved by 5yo)
- Fog test (walk on outside of feet then inside) exaggerates UMN signs inc flexion at arms
- Running (can exaggerate UNM lesions)
- Trendelenberg test (stand on one leg) dropping or compensatory rising opposite pelvis > proximal weakness
- Gowers manoeuvre LMN v Myopathic: sitting or supine > rolling prone first +/- using hands on thighs = position
Distal weakness heel/toe walking
4 main gaits (see youtube playlist)
- UMN
- hemiparetic (flexed, adducted, internally rotated, hip circumduction)
- with add shoulder, flex elbow, pronated wrist, thumbing of cortical fist
- Spastic diplegic (flexed adducted internal rotated hips, flexed knees, ankle ext, hyper circumduction
- with add shoulder, flexed elbows, pronated wrists
- hemiparetic (flexed, adducted, internally rotated, hip circumduction)
- Ataxic
- Widebased, truncal titubation, tandem gait exagerats
- Rhombergs (feet together eyes eyes open and sway > cerebellar, eyes shut > proprioception)
- Look for telangectasia
- Look for head/neck scars
- Neuropathic
- foot drop, high stepping compensation
- AHC: look for tongue fasciculations ?SMA
- Neuropathy: look for nerve thickening ? Charcot marie tooth
- NMJ: fatiguability ?Myasthenia gravy
- foot drop, high stepping compensation
- Myopathic
- Trendelenberg gait: waddle > pelvis drops on opposite side, hyperlordotic to balance
- Looks for biopsy, facial weakness, calf hypertrophy, scoliosis, cushingoid, alert for anaesthetic malignant hyperthermia)
- Proximal myopathy ?Muscular dystrophy look for intellectual impairment
- Myotonia ?myotonic dystrophy
- Trendelenberg gait: waddle > pelvis drops on opposite side, hyperlordotic to balance
----------------------------------------------
IF HEMI UMN DEFECT CHECK HEMIANOPIC VISUAL FIELD LOSS, HEMIATROPY AND LEG LENGTH DISCREPANCY!!!
If visual field defect, neglect, agnosia > cortical
If pure UMN > internal capsule
Upper motor neurone V LMN v Mixed (Leukodystrophy)
- Power/sensation/coordination ↓ in U or LMN
- Sensation - two point, graphesthesia, identify tissue, paperclip, coin
- simultaneous bilateral homologous - ?neglects one side (parietal)
- Romberg stand eyes arms out open (cerebellum) then closed (proprioception)
- UMN - ↓Intellect, ↑tone, ↑reflexes (pyramidal) ↑babinski, (ACUTELY LOOK LIKE LMN)
- Upper = above anterior horn
- Brain
- Bleed
- Ischemic stroke: Sickle, Infective endocarditis
- Haemorragic: Trauma, AVM, Aneurysm, Bleeding disorder
- Tumour
- Todd's Paresis
- Hemiplegic migraine
- Alternating hemiplegia of childhood
- Bleed
- Spinal cord
- Trauma
- Tumour
- Bleed
- Epidural abscess, Discitis
- Brown-Séquard syndrome = one side
- Weakness and posterior column (vib/prop) loss ipsil, anterior column (fine, pain , temp on contra)
- Anterior cord
- Weakness and lost of anterior column bilaterally with hypotension (sickle)df
- Brain
- Upper = above anterior horn
- LMN - N intellect ↓tone, ↓reflexes, fasciculations, wasting,
- Lower = anterior horn and below (AHC, NMJ and Muscular usually PROXIMAL weakness with intact sensation)
- AHC (SENSATION normal)
- Entero/Polio: asymmetric reduced tone
- SMA:
- Molecular genetics for SMN1 deletion
- Neuropathy (Sensation usually involved down/burning pain)
- Guillian Barré: ascending (heterogenous, can be demyelinating or axonal)
- Rabies
- Hypovitaminoses
- Medications, Pb, Mercury
- NMJ (SENSATION Normal, Fatigues, tone and reflexes often normal)
- Botilinum culture or toxin in stool/wound/blood
- ACh Receptor antibodies ?Myasthenia graves
- Snake bite (pre or post synapse)
- Tick paralysis (ascending)
- Muscle (SENSATION intact)
- AHC (SENSATION normal)
- Mixed
- Adrenleukodystrophy
- VLCFA
- MRI posterior white matter loss (T1 G is B W is W, hypointense)
- Adrenleukodystrophy
- Lower = anterior horn and below (AHC, NMJ and Muscular usually PROXIMAL weakness with intact sensation)
- Coordination (cerebellum is ipsilateral), gait (shoes) (Falls risk)
- maze toy
- Heel toe (>4yo)
Ix
Ask for RESULTS of genes, electromyogram, nerve conduction studies, muscle biopsy
- CK mild elevation in myopathy, significant in dystrophies
- Muscle panel usually done before painful nerve conduction/EMG as can give diagnosis
- Duchenne's dystrophin gene
- Nerve conduction (sensory, motor, ...) surface electrodes spaced along the nerve
- increase latency, or slow velocity think myelination, CMT, Schwann cells
- reduced amplitude, think loss of axons, think vincristine
- motor but not sensory (will have sensory deficit but post ganglion normal on sensory NCS as lesion is higher) think radiculopathy
- EMG
- adds muscle activity
- fibrillation can be nerve of muscle
- high amplitude fibrillation = acute pathology
- low amplitude = chronic
- recruitment reduced in neuropathy, increased in myopathy?
Acetylcholine receptor antibodies (Myasthenia)
UMN: tumour, bleed