Cardiology Examination
W
I
S
Exposure shirt off
Sitting then 45 from neck Ex on (can be on carers lap)
Equipt
Well
Growth
- short (T21, Williams, 22q11, Turners, Noonan)
- tall (Marfans/LDS)
- FTT (CHD)
Obs
Dys (T21, Williams, 22q11, Turners, Noonan, Marfans/LDS)
Well/unwell
WOB
Colour (Cynosis, Palour)
Alert
Skin
- bruising
Scars
Ex
Hand
Neck JVP <3cm, hepatojugular
Eyes
Summary
Cynotic v acynotic
Failure v not in failure
Peripherial finding
Paecardial findings
Syndromes
Ix
CXR: DRSABCDE
D: Details (name, age, AP film)
R: RIPE:
Rotation (clavicle:spinous process), Inspiration (8-10 post ribs), Picture (got entire lung fields), Exposure (spinous processes to T4, hemidiaphragm visible)
S: Soft tissues/bones – check fractures, swelling, calcificn
- butterfly vertebra (Alagille's)
A: Airway/mediastinum
B: Breathing:
Lung fields (collapse/consol, vascularity, lesions), Pleura (thickening)
C: Circulation (heart size, shape and borders)
D: Diaphragm (location, angles, gastric bubble, air under)
E: Extras – CVL lines etc.
ECG (NB 25mm/sec = 5 big boxes/sec is standard, 1mv =10mm (2 big boxes) is standard)
I
S
Exposure shirt off
Sitting then 45 from neck Ex on (can be on carers lap)
Equipt
Well
Growth
- short (T21, Williams, 22q11, Turners, Noonan)
- tall (Marfans/LDS)
- FTT (CHD)
Obs
Dys (T21, Williams, 22q11, Turners, Noonan, Marfans/LDS)
- if ?Marfans > gastrostomy/hypertelorism/bifid uvula = LD
Well/unwell
WOB
Colour (Cynosis, Palour)
Alert
Skin
- bruising
Scars
- Medial sternotomy (PA banding, Complex cardiac surg inc TOF, Bypass)
- posterolateral thoracotomy (BT(Blalock-Taussig) shunt, often reduced pulse on that side)
- left: PA banding, BT shunt, coarctation of the aorta, PDA ligation, OR Resp
- right PA banding, BT shunt OR, resp, TOFistula (VACTERL), Diaph hernia
- Chest drains
- Pacemaker
Ex
Hand
- cynosis
- clubbing (cyanotic heart disease)
- CR for perfusion
- palmar palour
- Infective endocarditis (janeway (painless palms)/splinter (nails)/oslers (painful palms)
- Tendon Xanthomata
- rate, rhythm (sinus arryth = inspiration drops vagal tone increased HR to maintain output)
- amplitude (reduced radial with coarc repair and BT shunts, reduced femoral with unrepaired coarc)
- character with wrist above heart (collapsing in AR)
- water hammer (tapping pulse in forearm muscles with arm elevate (AI)
- decrease left radial > repaired coarc or post BT shunt (look for L postlat thoracotomy)
- Decreased femorals > Coarct (Radiofemoral delay in adults)
- Paradoxus (exaggeration of normal drop in inspiration >10mmHg)
- look for femoral scars (angio)
Neck JVP <3cm, hepatojugular
Eyes
- Palor
- Jaundice (RHF, valve haemolysis)
- Xanthelasma
- Cranial bruit
- Mitral facies (chronic severe MR)
- Cynosis (compare with mum if unsure)
- Palate (high arched ?Marfans/turners, bifid uvula = LDS)
- Dentition (SBE)
- RR (up in pulm oedema from LHF)
- Left prominence with RVH, right with dextrocardia and VH
- Apex bilaterally (R ?Kartagener)
- Para/substernal heave
- suprasternal/supraclavicular thrill
- Palpable P2 at pulmonic area (PHTN)
- Auscultation starting at Mitral (Apex) S1 > systole > S2 > diastole, then bell for diastolic murmurs
- Mitral > roll left to accentuate
- Tricuspid (VSD)
- Pulm
- Ejection systolic (pulmonary flow inc ASD, RVOTO)
- supra has thrill (Pulm area or suprasternal notch)
- valvular has thrill + click
- subvalve has neither
- Ejection systolic (pulmonary flow inc ASD, RVOTO)
- Aortic
- Ejection systolic (LVOTO)
- supra has thrill
- valvular has thrill + click
- subvalve has neither
- Ejection systolic (LVOTO)
- Sounds (1,2)
- normal S2 splitting on inspiration
- fixed = septal defect
- no split = ?PHTN or isolated outflow
- Loud P2 = PHTN (Coarc, ..)
- Added (3,4)
- Click in mitral area > bicuspid AV
- Opening snap mitral stenosis
- Murmur
- Location
- Apex (MA)
- Systolic > radiating to axilla: MR (Cong: valve cleft/prolapse (Marfan's) /partial AVSD (T21), Acqu: IE/RHD), HOCM (Noonan)
- Diastolic > radiating to axilla: MS above not HOCM
- LLSE (TA):
- Systolic > VSD, TR
- Diastolic > TS
- LUSE (PA):
- Systolic > PS (Noonan)
- Post surg ?PA, PS, TOF/Truncus (22q11/di george)
- diastolic PR/PI to LLSE (PS and PI ?Repaired TOF)
- Systolic > PS (Noonan)
- RUSE (AA)
- Systolic to carotids > AS
- Supravalvular: Williams
- Valvular: RHD, Congenital bicuspid/unicuspid)
- Subvalvular: HOCM (Noonan)
- Diastolic
- AR/AI to LLSE: IE / RDH, Uni/Bicusp (Turners), Dilated root > AR (Marfans/Turners)
- Systolic to carotids > AS
- Continuous
- no cyanosis/club/scars
- PDA (unchanged with position/compression of ipsi IJVein)
- venous hum (supraclavicular, innocent) disappears on lying supine and on compression of ipsi IJV
- Shunt or major collaterals (eg Coarct (Turners), Pulm At with VSD)
- no cyanosis/club/scars
- Apex (MA)
- Grade
- No thrill
- barely heard
- soft
- easily
- Thrill
- easily heard
- with light steth
- with steth off chest
- No thrill
- radiation (ausc and palpate)
- mitral to axilla
- LVOTO to carotids
- supra has thrill
- valvular has thrill and click
- subvalve has neither
- Back: peripheral pulmonary stenosis, coarct
- Eyes/Fontanelle
- Location
- Sit forward: innocent diminish, pathological worse
- RILES Right side increase with insp, left sided increase with expiration
- Valsalva
- innocent decrease
- HOCM/MR increase
- Roll left to accentual mitral
- Lungs
- generalised creps ?LHF
- focal ? infection ? Kartageners
- Back
- Sacral oedema
- Abdo
- Pulsatile liver (TR)
- Hepatomegaly (RHF)
- Splenomegaly (SBE, Pompe's glycogen storage muscle breakdown)
- Renal bruit
- Groin scars
- Ankle oedema (RVF)
- Obs
- Temp (SBE)
- UA blood (SBE)
- Ophthalmoscopy
- Roths spots (haemorrhage with white centre SBE)
- Retinal haemorrhages (HTN)
Summary
Cynotic v acynotic
Failure v not in failure
Peripherial finding
Paecardial findings
Syndromes
Ix
CXR: DRSABCDE
D: Details (name, age, AP film)
R: RIPE:
Rotation (clavicle:spinous process), Inspiration (8-10 post ribs), Picture (got entire lung fields), Exposure (spinous processes to T4, hemidiaphragm visible)
S: Soft tissues/bones – check fractures, swelling, calcificn
- butterfly vertebra (Alagille's)
A: Airway/mediastinum
B: Breathing:
Lung fields (collapse/consol, vascularity, lesions), Pleura (thickening)
C: Circulation (heart size, shape and borders)
D: Diaphragm (location, angles, gastric bubble, air under)
E: Extras – CVL lines etc.
ECG (NB 25mm/sec = 5 big boxes/sec is standard, 1mv =10mm (2 big boxes) is standard)
- Rate
- Rhythm – regular/irregular/sinus
- Axis: I and AVF
- Pwave
- tall RAE (>2.5mm or 2.5 smalls)
- wide/bifid LAE (>120ms or 3 smalls)
- PR interval: P waves: QRS – before each QRS?
- Block: 1st degree – prolonged PR
- Block: 2nd degree:
- Mobitz I: progressive lengthening PR then dropped beat (Wenkeback)
- Mobitz II: 2:1 HB – 2 or 3 p’s for each QRS
- Block: 3rd degree: complete heart block - no relation between the P wave and the QRS complex
- Q waves: allowed in I, II, III and aVF, pathological in V1 (HOCM)
- QRS complex:
- RAD, tall R in V1, deep S in V6 = RVH
- LAD, deep S (>25mm) V1, tall R in V6 = LVH (esp combined with inverted T in V6 = strain)
- ST segment – elevation/depression, upslope,downslope
- T wave – peaked, inverted
- QT interval - <440 male <450 female.
- Karyotype: T21,

T21: AVSD

Williams: supravalvular AS, but can be any artery stenosis eg peripheral pulm, renal, thoracic aorta.. High Ca, renal anomalies
FISH for 7q11.23 deletion
FISH for 7q11.23 deletion

Noonans: hypertelorism, downward eye slant, and low-set ears, short, pulmonary stenosis
Geneticist for clinical diagnosis
Noonan's Syndrome panel (60% have identified gene)
Geneticist for clinical diagnosis
Noonan's Syndrome panel (60% have identified gene)
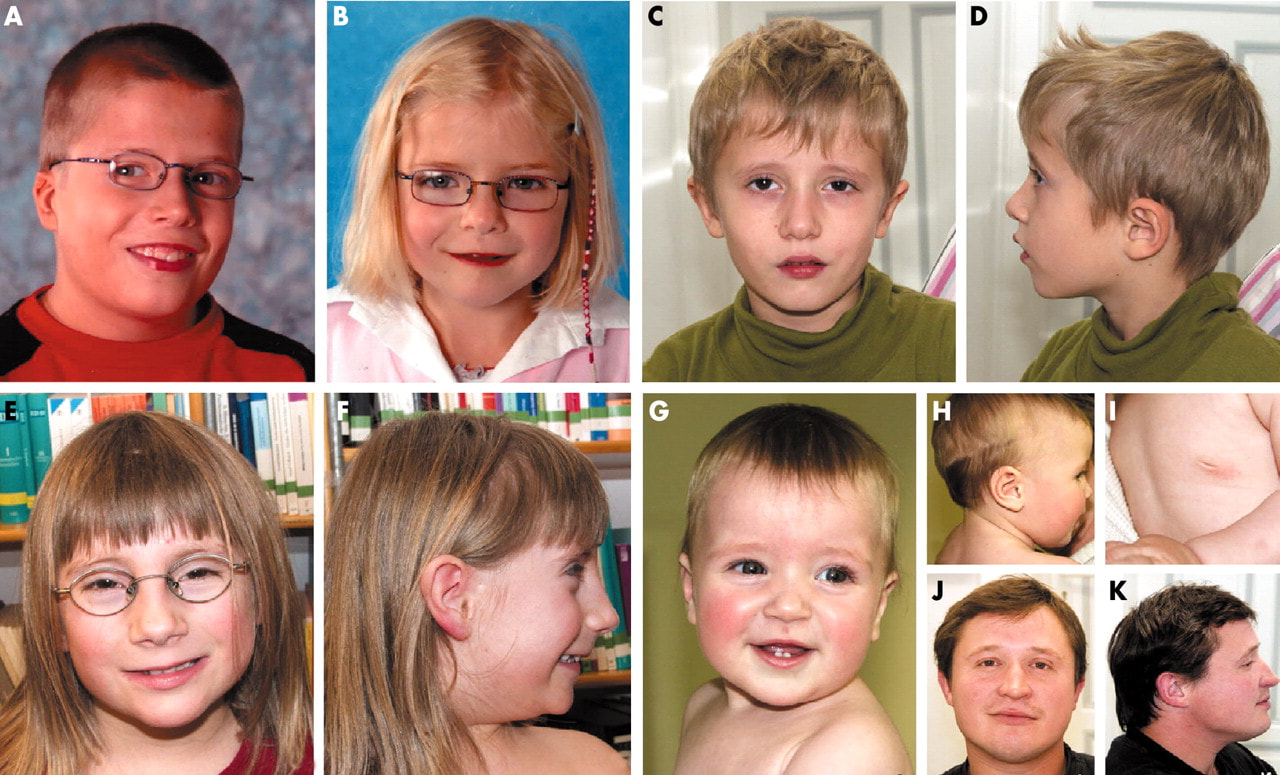
Turner's Syndrome: short, webbed neck, wide spaced nipples, Coarctation, bicuspid aortic valve
Karyotype for XO
Karyotype for XO
22q11.2 deletion syndrome (Di George, VCFS): thin upper lip, smooth philtrum, low set ears (interrupted arch, trunks arteriosus, TOF, ASD/VSD, vascular ring. hypo
FISH
hypocalcaemia from hypoparathyroidism, T-cell count
FISH
hypocalcaemia from hypoparathyroidism, T-cell count

Marfan's: Mitral valve prolapse leading to MR and HF. Ectopia lentis
Marfan panel (Marfans FBN1, Looeys-Dietz, familial thoracic aortic aneurysms and dissections
Marfan panel (Marfans FBN1, Looeys-Dietz, familial thoracic aortic aneurysms and dissections

Loeys-Dietz: similar to Marfan's, hypertelorism, split uvula, risk of aortic dilation

Alagille syndrome: triangular, deep set eyes, prominent forehead (peripheral pulm artery stenosis > TOF/DA/septal defects), butterfly vertebra
Dx, Sequencing for JAG1 (90%), then NOTCH2 if neg
Dx, Sequencing for JAG1 (90%), then NOTCH2 if neg
MURMURS
Ejection systolic (heard loudest above the nipple line)
Mid-diastolic
Ejection systolic (heard loudest above the nipple line)
- With a carotid thrill = left ventricular outflow tract obstruction
- Without a carotid thrill = right ventricular outflow tract obstruction
- Pulmonary stenosis – harsh, radiates to back, systolic click (variable i.e. decreases with inspiration), soft P2, fixed widened splitting of S2
- Atrial septal defect – harsh, fixed widened splitting of S2 and systolic pulmonary flow murmur
- Coarctation - radiates to the back (left interscapular area); decrescendo diastolic murmur at the third left intercostal space (aortic regurgitation from a bicuspid aortic valve), thrill at the suprasternal notch, ejection click at the apex - upper limb blood pressure is greater than lower limb blood pressure (if >20 mmHg then the desceding aorta is less than one third of the normal diameter), leg pulses weak/absent/delayed
- Innocent pulmonary flow
- Aortic stenosis (valvular) – radiates to carotids, ejection systolic click; decrescendo diastolic murmur at the third left intercostal space (aortic regurgitation from a bicuspid aortic valve or in discrete subvalvular stenosis)
- Aortic stenosis (supravalvular) - with radiation to the neck/apex, right arm blood pressure is greater than the left arm blood pressure, no ejection click
- Right BT shunt
- Mitral regurgitation
- Tricuspid regurgitation
- Ventricular septal defect
- Ventricular septal defect - early systolic murmur (if muscular) or pansystolic (if perimembranous) at LLSE; MDR in the apex (relative mitral stenosis); decrescendo diastolic murmur at upper right sternal edge (aortic regurgitation)
- Still’s murmur - louder with postural drop, musical
- Atrioventricular septal defect – superior axis
- Hypertrophic obstructive cardiomyopathy – cardiomegaly, deep Q waves
- Tricuspid regurgitation
- Mitral regurgitation
- Ventricular septal defect
- Vibratory innocent murmur
- Mitral valve prolapse
- Aortic stenosis
- Mitral stenosis
- Patent ductus arteriosus – with bounding pulses
- Arteriovenous fistula
- Persistent truncus (rare)
- BT Shunt – check for scars
Mid-diastolic
- Tricuspid stenosis - best heard at lower left sternal edge - associated with atrial septal defect, TAPVR, endocardial cushion defect
- Mitral stenosis - best heard at the apex - associated with a large left-to-right shunt in a ventricular septal defect, patent ductus arteriosus
- Pulmonary regurgitation - best heard at the third left intercostal space - post pulmonary stenosis/right ventricular outflow tract obstruction surgery
- Aortic regurgitation - best heard at the third left intercostal space (directed towards the apex)