Iron Deficiency
Summeried Nelson but need to add fig 449-1/2
Most common nutritional disorder in the world (30% prevalence of iron def. ANAEMIA!)
most common 9-24mo
Intense exercise may contribute to deficiency in girls
Some normal iron loss in shedding of cells
Pathophysiology:
0.5g of iron in neonate
<10% absorption = 10mg/day RDI
2-3 x better absorbed from human milk than cow
Developing world = problem of inadequate intake of Fe rich foods
Developed world = to much dairy (less absorbed plus losses from milk protein colitis)
Absorbed in duodenum
NB Can have irreversible effects on cognitive and motor function before microcytosis or anaemia develops
Intake or
Chronic blood loss:
Meckel's
Peptic ulcer
polyp
haemangioma
IBD
Menstral loss
Pregnancy
Exercise (haematuria, haemolysis)
Protein colitis (limit cows milk to 700ml/d and only in >1yo)
Infection
Hx
Pica - non-nutritous cravings
Pagophagia - ice craving
(Hb <50)
Irritability
Anorexia
lethargy
Anaemia
Breathholding
Idiopathic intracranial hypertension (aka BIH, aka Pseudotumour cerebri)
Restless legs / periodic leg movement disorder
Ex
Pallor of palmar creases/palms/nailbeds/conjunctivae when Hb<80
Systolic flow murmur
Tachycardia
High output failure
Ix
Stool for occult blood and parasites
Microcytic anaemia with ↑red cell distribution width (RDW not ↑ in thalassemias)
Iron binds to protoporphyrins to produce heme
Less heme (↓MCH/hypochromic) > microcytosis (↓MCV) > ↑ RDW (anisocytosis)
They are more fragile > ↓RBC/Hb > Reticulocytosis
Film: above plus, elliptocytic
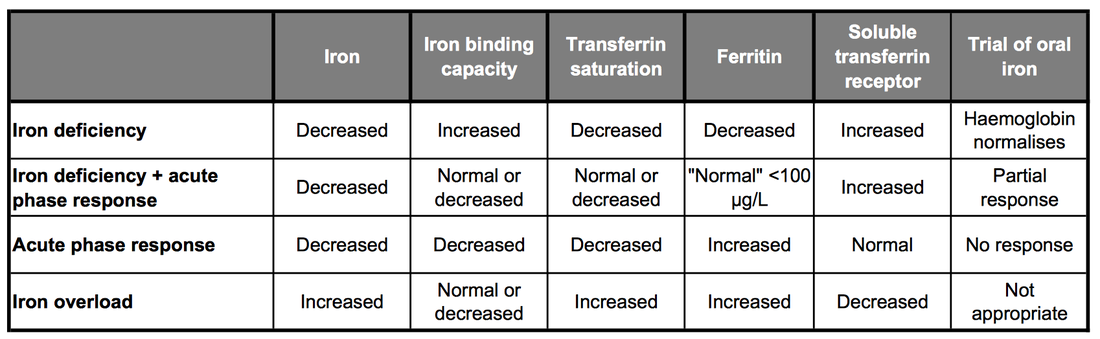
Ferritin (intracellular iron storage protein) gives a good indication of iron stores in the absence of inflammation
Serum iron decreases
transferrin (serum iron storage protein) increases
Total iron binding capacity (inexpensive surrogate for transferrin level) increases
Transferrin saturation drops
If indices indicate iron deficiency BUT ferritin is not low ?mixed acute phase >
Transferrin receptor (internalises transferrin:iron complex into cells) increases
If pica present check Pb level (Plumbism)
If microcytic anaemia and RDW ↑
Rx
PO iron, reticulocyte count response in 72hours!
If no response
?DDx
Most common nutritional disorder in the world (30% prevalence of iron def. ANAEMIA!)
most common 9-24mo
Intense exercise may contribute to deficiency in girls
Some normal iron loss in shedding of cells
Pathophysiology:
0.5g of iron in neonate
- in Hb at birth, some reclaimed as Hb drops, lasting 6-9m
- delayed cord clamping can improve this in at risk groups
<10% absorption = 10mg/day RDI
2-3 x better absorbed from human milk than cow
Developing world = problem of inadequate intake of Fe rich foods
Developed world = to much dairy (less absorbed plus losses from milk protein colitis)
Absorbed in duodenum
NB Can have irreversible effects on cognitive and motor function before microcytosis or anaemia develops
Intake or
Chronic blood loss:
Meckel's
Peptic ulcer
polyp
haemangioma
IBD
Menstral loss
Pregnancy
Exercise (haematuria, haemolysis)
Protein colitis (limit cows milk to 700ml/d and only in >1yo)
Infection
- Hook worm
- Trichuris trichiura (Whip worm)
- Plasmodium (Malaria)
- H Pylori
Hx
Pica - non-nutritous cravings
Pagophagia - ice craving
(Hb <50)
Irritability
Anorexia
lethargy
Anaemia
Breathholding
Idiopathic intracranial hypertension (aka BIH, aka Pseudotumour cerebri)
Restless legs / periodic leg movement disorder
Ex
Pallor of palmar creases/palms/nailbeds/conjunctivae when Hb<80
Systolic flow murmur
Tachycardia
High output failure
Ix
Stool for occult blood and parasites
Microcytic anaemia with ↑red cell distribution width (RDW not ↑ in thalassemias)
Iron binds to protoporphyrins to produce heme
Less heme (↓MCH/hypochromic) > microcytosis (↓MCV) > ↑ RDW (anisocytosis)
They are more fragile > ↓RBC/Hb > Reticulocytosis
Film: above plus, elliptocytic
Ferritin (intracellular iron storage protein) gives a good indication of iron stores in the absence of inflammation
Serum iron decreases
transferrin (serum iron storage protein) increases
Total iron binding capacity (inexpensive surrogate for transferrin level) increases
Transferrin saturation drops
If indices indicate iron deficiency BUT ferritin is not low ?mixed acute phase >
Transferrin receptor (internalises transferrin:iron complex into cells) increases
If pica present check Pb level (Plumbism)
If microcytic anaemia and RDW ↑
Rx
PO iron, reticulocyte count response in 72hours!
If no response
?DDx