Dentition
See also Dental Prevention
Australasian Academy of Paediatric Dentistry
General Dentist
Endodontist = specialist in root canal surgery
Periodontist = specialist in gum disease
Prosthodontist = specialist in prosthetics
Orthodontist = specialist in straightening
Begins in embryogenesis week 6
Use of tetracylines during development (week 18 to 8years) can cause grey staining of developing teeth
Primary 2-6yo (20)
Eruption (shed)
Teething
Can oscillate i.e. come in and out before finally coming through
No evidence for any symptoms (fever, irritability, dehydration, hypersalivation, skin eruptions, flushed, ear pulling, GIT disturbance)
Rx ?cool chewing ring (not frozen), analgesia, fluids
Bruise over eruption = Eruption haematoma (benign, no Rx)
Ectodermal displasia (look at hair, skin, nails)
Effects nutrition which effects physical and cognitive development
Quality of life
Painfree
Asthetics, self esteem
Masticatory function
Ex
Parent and doctor facing each other
Childs legs around parent facing them
Parents hold arms and child lays back along parents legs and doctors legs
Open wide
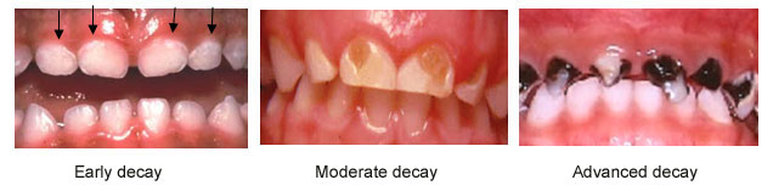
Early childhood caries (i.e. <6yo)
aka nursing bottle mouth/baby bottle tooth decay/bottle caries/nursing caries
Poor hygiene > caries
Infection > poor sleep > familial stress > bottle to settle > caries
Tasting/Sharing of food > introduces bacteria
Early tooth eruption > earlier opportunity for bacteria adhesion
Bronchodilators > dry teeth, leave a film Rx rinse with any inhaler
Bacterial fermentation of food creates acid
White demineralisation close to gum is the early sign
Prevalence 25% at 3y, 50% at 5y
Prognosis: early to advanced in months
can cause facial cellulitis (periorbital, submandibular...)
Rx
Preventative dental hygiene
OT for extraction or drainage and root canal
Amp, metronidazole
No dummies,
Minimise sugar
Stimulate salivation with lozenge/sugar free gum
No smoking (reduces saliva)
?Collis curve toothbrush
Bottle > Cup feeding as soon as able
No putting to bed with milk
Stop breast feeding by 2yo
Stop bottle feeding by 1yo (if require a period to weaning behaviour, water only)
?probiotic
Tooth mousse
Screen for obesity, DMT2
Microbiology
Supragingival i.e. caries
Subgingival (between tooth and gum) i.e. gingivitis
Gingivitis
BD floss, brush, and fluoride mouth wash
6monthly dentist removal of plaque
Non-alcoholic chlorhexidine mouthwash for severe cases
Acute ulcerative gingivitis augmentin or clindamycin for 5 days
Tooth erosion
Tongue rings
Fluorosis
Ectodermal dysplasia
Extra oral draining sinus
Neonatal tooth
Laminar cyst: keratin filled epithelial remnant, self resolve
Congenital epulis
Riga-Fede disease
Gingival eruption cyst
Mucocele: salivary retention cyst (ranula if in floor of mouth)
Sialolith: salivary stone
Orofacial granulomatosis (collection of macrophages)
Chronological enamel hypoplasia
Ulcers:
Amylogenesis imperfecta
Trauma
?Impaction
?alveolar fracture
?laceration
No need to replant primary teeth
Mouthguard!
Avulsion > replace (5-10mins), or in milk if cannot, Rx splinting and antibiotics
Take in pieces! (check lip) can be bonded
Frenulum
Fluoride in drinking water is low dose, does not cause fluorosis
unrelated
OM
herpangina
primary HSV
Gastro
Meningitis
Australasian Academy of Paediatric Dentistry
General Dentist
Endodontist = specialist in root canal surgery
Periodontist = specialist in gum disease
Prosthodontist = specialist in prosthetics
Orthodontist = specialist in straightening
Begins in embryogenesis week 6
Use of tetracylines during development (week 18 to 8years) can cause grey staining of developing teeth
Primary 2-6yo (20)
- Upper right = quadrant 5
- Upper left = quadrant 6
- Lower left = quadrant 7
- Lower right = quadrant 8
- Ugly duckling phase
- Upper right = quadrant 1
- Upper left = quadrant 2
- Lower left = quadrant 3
- Lower right = quadrant 4
Eruption (shed)
- Lower central incisor 6-10m (6-7y)
- Upper central incisor 8-12m (6-7y)
- Upper lateral incisor 9-13m (7-8y)
- Lower lateral incisor 10-16m (7-8y)
- Upper 1st molar (3cusps) 13-19m (premolar/bicuspid 9-11y)
- Lower 1st molar (4cusps) 14-18m (premolar/bicuspid 9-11y)
- Upper canine/cuspid 16-22m (10-12y)
- Lower canine/cuspid 17-23m (9-12y)
- Lower 2nd molar 23-31m (premolar/bicuspid 10-12y)
- Upper 2nd molar 25-33m (premolar/bicuspid 10-12y)
- 1st (quadrate) molars 6-7y (6yo molar)
- 2nd (quadrate) molars 11-13y (12yo molar)
- 3rd (quadrate) molars 17-21y (Wisdom teeth)
Teething
Can oscillate i.e. come in and out before finally coming through
No evidence for any symptoms (fever, irritability, dehydration, hypersalivation, skin eruptions, flushed, ear pulling, GIT disturbance)
Rx ?cool chewing ring (not frozen), analgesia, fluids
Bruise over eruption = Eruption haematoma (benign, no Rx)
Ectodermal displasia (look at hair, skin, nails)
Effects nutrition which effects physical and cognitive development
Quality of life
Painfree
Asthetics, self esteem
Masticatory function
Ex
Parent and doctor facing each other
Childs legs around parent facing them
Parents hold arms and child lays back along parents legs and doctors legs
Open wide
Early childhood caries (i.e. <6yo)
aka nursing bottle mouth/baby bottle tooth decay/bottle caries/nursing caries
Poor hygiene > caries
Infection > poor sleep > familial stress > bottle to settle > caries
Tasting/Sharing of food > introduces bacteria
Early tooth eruption > earlier opportunity for bacteria adhesion
Bronchodilators > dry teeth, leave a film Rx rinse with any inhaler
Bacterial fermentation of food creates acid
White demineralisation close to gum is the early sign
Prevalence 25% at 3y, 50% at 5y
Prognosis: early to advanced in months
can cause facial cellulitis (periorbital, submandibular...)
Rx
Preventative dental hygiene
OT for extraction or drainage and root canal
Amp, metronidazole
No dummies,
Minimise sugar
Stimulate salivation with lozenge/sugar free gum
No smoking (reduces saliva)
?Collis curve toothbrush
Bottle > Cup feeding as soon as able
No putting to bed with milk
Stop breast feeding by 2yo
Stop bottle feeding by 1yo (if require a period to weaning behaviour, water only)
?probiotic
Tooth mousse
Screen for obesity, DMT2
Microbiology
Supragingival i.e. caries
- gram positive feeding on food (Strep mutans)
- Salivary IgA not efficient at killing
- Cause caries when pathogens overgrow non-pathogenic bacteria
- cause of overgrowth include acidic and sugar intake, low saliva
Subgingival (between tooth and gum) i.e. gingivitis
- gram negative feeding on nutrients in crevicular fluid
- Attacked by IgGME (so ?vaccinate)
- Cause gingivitis, peridontitis
Gingivitis
- Plaque, if left, forms calculus (aka tartar)
- Swollen, bleeding gums (reaction to calculus)
- Halitosis
- Loose teeth
BD floss, brush, and fluoride mouth wash
6monthly dentist removal of plaque
Non-alcoholic chlorhexidine mouthwash for severe cases
Acute ulcerative gingivitis augmentin or clindamycin for 5 days
Tooth erosion
- Looks like they have been grinding
- Acid drinks
- GORD
- Thick frothy saliva
Tongue rings
- nerve damage to tongue
- Acute trauma to tooth i.e. bite down and chip off a cusp
Fluorosis
- White streak on teeth from swallowing large amounts of fluoride toothpaste
Ectodermal dysplasia
- Pointy incisors
Extra oral draining sinus
- think tooth abscess
Neonatal tooth
- Familial
- superficially place deciduous tooth that has erupted early, may not have root structure, often loose
- Risk of ulceration, poor feeding, aspiration
- Rx dentist for removal
Laminar cyst: keratin filled epithelial remnant, self resolve
- Epstein pearl if on palate
- Bohn nodule if on gum
Congenital epulis
- benign tumour, Rx resection
Riga-Fede disease
- sublingual ulceration
- ? congenital neuropathy e.g. Riley Day, Lesch-Nyhan
Gingival eruption cyst
- cyst over erupting tooth
Mucocele: salivary retention cyst (ranula if in floor of mouth)
- Rx Marsupialisation
Sialolith: salivary stone
Orofacial granulomatosis (collection of macrophages)
- swollen lips and gums
- can be precursor to Crohn's
Chronological enamel hypoplasia
- systemic event during development transiently effecting amyloblasts
Ulcers:
- Primary herpes
- Hand foot and mouth
- Aphthus
Amylogenesis imperfecta
- genetic protein defect
- effects all teeth
Trauma
?Impaction
- OPG by dentist to establish if abutting permanent tooth. Rx removal to prevent enamel damage
?alveolar fracture
?laceration
No need to replant primary teeth
Mouthguard!
Avulsion > replace (5-10mins), or in milk if cannot, Rx splinting and antibiotics
Take in pieces! (check lip) can be bonded
Frenulum
- superior: no Rx will recede with age
- sublingual if interfering with feeding
Fluoride in drinking water is low dose, does not cause fluorosis
unrelated
OM
herpangina
primary HSV
Gastro
Meningitis