Bladder Dysfunction
Urine storage
infants void 15-20 times/day
Expected bladder capacity (ml): (Age + 2) x 30
Continence
Toilet training can commence ~2-4yo, transition phase is between commencement and achievement
bowel control comes before bladder control
Girls earlier than boys
Requires:
Incontinence
Hx of incontinence
Pattern
Volume
Stream strong
Vincents curtsy (squatting on foot to prevent incontinence)
Constant leak
Sensation of incomplete emptying
UTIs
Reflux
Neurological disorder
Constipation
FH duplication
Hx SAbuse
Ex
Short stature
HTN
Palpable kidneys/bladder
Faecolith
Labial adhesions
urethral ectopy
Back/sacral anomaly
LL neuro
Ix
UA, MCS
Bristol
Bladder diary: time, volume, wet/dry
Post void residual (bladder scan): Positive in overactive bladder
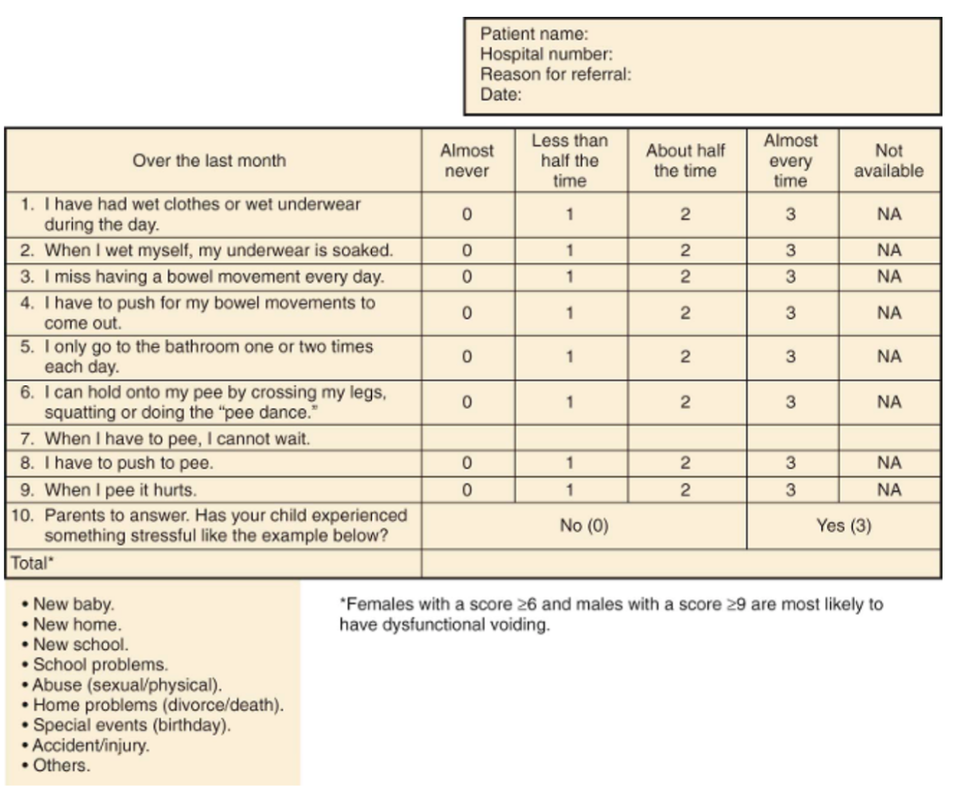
Dysfunctional voiding score (see below)
Uroflow (noninvasive assessment of urinary flow pattern) with or without EMG (measurement of external sphincter activity)
MCUG: spinning top (dilated proximal urethra = overactive bladder)
Urodynamics if neurologic disease OR unresponsive to empirical therapy
Keep diary of above
Diurnal incontinence
5yo = 92% are dry during day
7yo = 96% are dry during day (15% have significant urgency at times)
12yo = 99% are dry during day
Daytime incontinence
Most common: overactive bladder: strong uninhibited bladder contraction with inadequate relaxation of the external sphincter
Rx timed voiding 90m-2hrly, Kegel pelvic floor exercises, anticholinergic (oxybutynin)
Treatment
alphaadrenergic antagonist for NNDV i.e. abnormal sphincter tone
ADH analogue is 2nd line for nocturnal enuresis (desmopressin)
TCA imipramine is 3rd line for nocturnal enuresis
Giggle
Large volume loss with laughing in girls
proposed etiology similar to cataplexy i.e. involuntary hypotonia of external sphincter
other thought is related to detrusor instability
another is CNS
Rx multiple have been show to give improvement
anticholinergic (detrusor)
methylphenidate (CNS)
biofeedback with external sphincter exercises
Enuresis: incontinence in sleep in >5yo
Primary
Secondary
Non-monosymptomatic Nocturnal Enuresis
Causes: constipation, overactive bladder, poor sleep arousal, small bladder capacity, nocturnal polyuria
Demystify and education
remove blame
40% fluid <1200, 40% 12-1700, 20% >1700
Avoid sugar and caffeine generally, avoid fluid and solutes in evening
treat constipation
Urine culture and glucose
If post void residual > specialist
If overactive bladder (frequency, urgency, urge incontinence) > Oxybutinin (anticholinergic) for 12m, add alarm if no response
- sympathetic and pudendal nerve-mediated
- inhibition of detrusor contractile activity
- closure of the bladder neck and proximal urethra with increased activity of the external sphincter
- reflex bladder contraction
- simultaneous coordinated relaxation of the sphincter
infants void 15-20 times/day
Expected bladder capacity (ml): (Age + 2) x 30
Continence
Toilet training can commence ~2-4yo, transition phase is between commencement and achievement
bowel control comes before bladder control
Girls earlier than boys
Requires:
- normal bladder growth
- awareness of full bladder
- voluntary control of bladder to prevent incontinence until at toilet
- cortical inhibition (suprapontine modulation) of reflex (unstable) bladder contractions
- voluntary external sphincter contraction
- motivation by the child to stay dry
Incontinence
- Neurological
- neurology, cutaneous signs of occult spinal dysraphism or sacral agenesis, or a history of perinatal/neonatal injury
- Anatomical
- weak stream (posterior urethral valves)
- Functional
- Overactive bladder: urgency
- Non-neurogenic dysfunctional voiding
- unable to relax the urethral sphincter and/or pelvic floor musculature during voids
- often have constipation resulting in bowel-bladder dysfunction (aka dysfunctional elimination syndrome)
- Voiding postponement: voluntarily postponing
- low frequency, large volume voids
- holding maneuvers to suppress voiding.
- Underactive bladder: voiding postponement leads underactive bladder
- poor or absent bladder contraction
- straining (eg, Valsalva maneuver)
- weak and interrupted urinary stream
- Rx behavioral therapeutic interventions aimed at retraining the bladder and urinary sphincter
Hx of incontinence
Pattern
- day v night
- Urgency
- Giggle
Volume
Stream strong
Vincents curtsy (squatting on foot to prevent incontinence)
Constant leak
Sensation of incomplete emptying
UTIs
Reflux
Neurological disorder
Constipation
FH duplication
Hx SAbuse
Ex
Short stature
HTN
Palpable kidneys/bladder
Faecolith
Labial adhesions
urethral ectopy
Back/sacral anomaly
LL neuro
Ix
UA, MCS
Bristol
Bladder diary: time, volume, wet/dry
Post void residual (bladder scan): Positive in overactive bladder
Dysfunctional voiding score (see below)
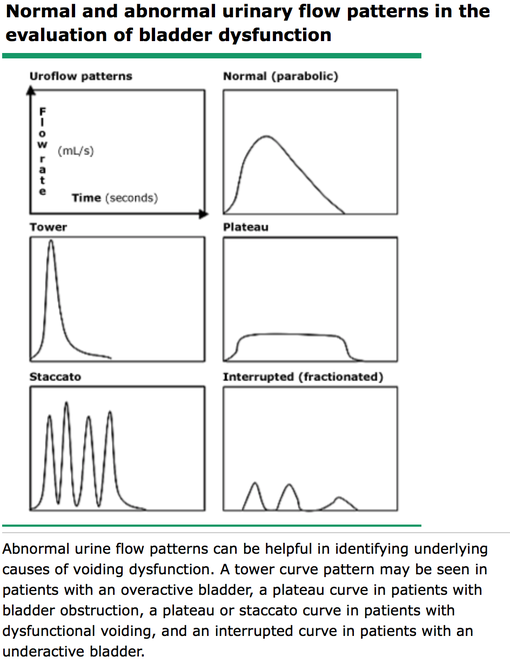
Uroflow (noninvasive assessment of urinary flow pattern) with or without EMG (measurement of external sphincter activity)
- Gives information of emptying but not filling phase
- Wait until strong desire to void (ideally until urgency) (100ml minimum)
- Void into device that produces urine flow curve
- shape of flow
- void volume
- void time
- maximum flow (Qmax)
- average flow
- electromyographic activity of the urethral sphincter and pelvic floor musculature can be assessed using pads affixed to the perineum. Sphincter activity should be absent during voiding.
- Bladder capacity = void volume + post void residual (US)
- ↓(vs expected) in overactive
- ↑ (vs expected) in underactive
MCUG: spinning top (dilated proximal urethra = overactive bladder)
Urodynamics if neurologic disease OR unresponsive to empirical therapy
- Urethral and rectal catheters to assess detrusor and sphincter function during filling AND voiding
- Overactive: involuntary detrusor contractions during filling (high filling pressure) normal set void, normal sphincter
- i.e. overactive = abnormal detrusor contraction against normal sphincter contraction in filling
- Non-neurogenic dysfunctional voiding: Normal detrusor during fill/void, norm sphincter in fill, abnormal sphincter tone in void
- i.e. dysfunctional = normal detrusor contraction against abnormal sphincter tone in void
- Underactive: large capacity, post void residual, normal sphincter
- Overactive: involuntary detrusor contractions during filling (high filling pressure) normal set void, normal sphincter
Keep diary of above
Diurnal incontinence
5yo = 92% are dry during day
7yo = 96% are dry during day (15% have significant urgency at times)
12yo = 99% are dry during day
Daytime incontinence
Most common: overactive bladder: strong uninhibited bladder contraction with inadequate relaxation of the external sphincter
Rx timed voiding 90m-2hrly, Kegel pelvic floor exercises, anticholinergic (oxybutynin)
Treatment
- Overactive bladder: 1) conservative measures (ie, timed voiding and treatment for constipation) 2) anticholinergic agent
- Underactive bladder: 1) Timed voiding + 2) double-voiding if post-void residual 3) line: clean intermittent catheterization NB Avoid Anticholinergics (increase post-void)
- Non-neurogenic dysfunctional voiding: 1) refer to urologist for urodynamics 2) pelvic floor relaxation measures 3) biofeedback 4) alpha antagonist.
alphaadrenergic antagonist for NNDV i.e. abnormal sphincter tone
ADH analogue is 2nd line for nocturnal enuresis (desmopressin)
TCA imipramine is 3rd line for nocturnal enuresis
- reduced time in REM sleep
- stimulated ADH secretion
- relaxes detrusor
Giggle
Large volume loss with laughing in girls
proposed etiology similar to cataplexy i.e. involuntary hypotonia of external sphincter
other thought is related to detrusor instability
another is CNS
Rx multiple have been show to give improvement
anticholinergic (detrusor)
methylphenidate (CNS)
biofeedback with external sphincter exercises
Enuresis: incontinence in sleep in >5yo
Primary
Secondary
Non-monosymptomatic Nocturnal Enuresis
Causes: constipation, overactive bladder, poor sleep arousal, small bladder capacity, nocturnal polyuria
Demystify and education
remove blame
40% fluid <1200, 40% 12-1700, 20% >1700
Avoid sugar and caffeine generally, avoid fluid and solutes in evening
treat constipation
Urine culture and glucose
If post void residual > specialist
If overactive bladder (frequency, urgency, urge incontinence) > Oxybutinin (anticholinergic) for 12m, add alarm if no response
- focusing on daytime symptoms first then nocturnal
- Timed voiding