Renal Failure
Insufficiency
Diuretic
Fluid restriction
Dialysis
K+ high in acute, compensates overtime
large kidneys on US (v small in chronic)
pre-renal, intrinsic, post renal (stone, Post Uret Val)
intrinsic: tubular, glomerular, vascular, C3
Urine osmo tells you if it is prerenal i.e. if >500 = can concentrate = prerenal
urine Na <20 = resorbing = prerenal
Ur:Pl Cr >40 = can concentrate = prerenal
Fractional excretion of Na = (UNa x PCr) / (UCr x PNa) x 100 = <1
otherwise ?ATN
Acute renal failure differentiation
Fractional excretion of sodium = Na excreted / Na filtered = UNa x Vol / Serum Na x Cr Clearance
AKI
Prerenal = most common cause
ATN =
Tumour lysis syndrome
Cortical necrosis (ischaemia particularly neonatal hypoxia, ...)
papillary necrosis (Sickle, ..)
Rx
Hypovolaemic > IV fluids/albumin
Hypervolaemic > fluid restriction, ?frusemide to optimise the functioning nephrons
Renal replacement therapy
indications
Haemofiltration: pressure pushes water and solutes through filter, these are discarded, water and electrolytes are replaced
Dialysis: diffusion across a membrane, with haemodialysis, large volume of extracorporeal blood i.e. not feasible in critical pts
Haemo:
Peritoneal:
Chronic:
compensation
increased excretion per functional nephron
reduced tubular resorption
PTH high in chronic
Low Ca
High PO4
reduced growth
anaemia
osteopenia
small kidneys on US (v large in acute)
if minimal haematuria / proteinuria
Acute ? Tubular interstitial nephritis (ibuprofen, antibiotics)
Chronic tubulointerstitial nephritis:
Note of cystic Kidney disease (ARPKD, ADPKD, NPHP, ADTKD)
Acute Renal Failure/Insufficiency = pRIFLE
Kidney Disease Improving Global Outcomes (KDIGO) acute kidney injury
Chronic Kidney Disease = GFR <60ml/min/1.73m2 for >3m
End-stage Renal Disease = those on renal replacement therapy i.e. dialysis or transplanted
Slowing progression
Complications
Hyperkalemia
Diuretic
Fluid restriction
Dialysis
K+ high in acute, compensates overtime
large kidneys on US (v small in chronic)
pre-renal, intrinsic, post renal (stone, Post Uret Val)
intrinsic: tubular, glomerular, vascular, C3
Urine osmo tells you if it is prerenal i.e. if >500 = can concentrate = prerenal
urine Na <20 = resorbing = prerenal
Ur:Pl Cr >40 = can concentrate = prerenal
Fractional excretion of Na = (UNa x PCr) / (UCr x PNa) x 100 = <1
otherwise ?ATN
Acute renal failure differentiation
- Urine osmolality normal (>400 mOsm/kg, spec grav >1.020), Ur Na normal (<20 mEq/L, frac exc <1% or 2.5 for neon)
- Urine protein normal/low > prerenal ie hypovolaemia (Or acute obstruction)
- Urine protein high (>100mg/dL) > Glomerulonephritis
- Urine osmolality low (<350 mOsm/kg, Spec grav <1.010), Ur Na high (>30 mEq/L, frac exc >1% or 10 for neon)
- Tubular: Acute tubular necrosis (Brown muddy granular casts), Fanconi Syndrome, Bartter, Gitelman, Little's
- Interstitial: Acute interstitial nephritis (WC/Eo casts)(pyelonephritis) often a hypersensitivity (eosinophils) to inf/drugs
Fractional excretion of sodium = Na excreted / Na filtered = UNa x Vol / Serum Na x Cr Clearance
- simplifies to: Ur Na x Serum Cr / Serum Na x Ur Cr x 100
AKI
Prerenal = most common cause
ATN =
Tumour lysis syndrome
Cortical necrosis (ischaemia particularly neonatal hypoxia, ...)
papillary necrosis (Sickle, ..)
Rx
Hypovolaemic > IV fluids/albumin
Hypervolaemic > fluid restriction, ?frusemide to optimise the functioning nephrons
Renal replacement therapy
indications
- Fluid overload unresponsive to fluid restriction/frusemide or with CCF/Pulm oedema/refractory HTN
- Hyperkalaemia unresponsive to nondialytic measures
- Uremia >?
Haemofiltration: pressure pushes water and solutes through filter, these are discarded, water and electrolytes are replaced
Dialysis: diffusion across a membrane, with haemodialysis, large volume of extracorporeal blood i.e. not feasible in critical pts
Haemo:
Peritoneal:
- Modality
- Manual: continuous ambulatory PD = keep bags with you, 4 exchanges i.e. 3 day cycles and one night
- Automatic:
- Night intermittent: automated cycles overnight, nil day dwell
- Continuous cycling PD: automated overnight, with day dwell
- Contain H2O, electrolytes, acid buffer (lactate, acetate or HCO3), and dextrose (1.5, 2.5, and 4.25%) for osmotic draw of H2O
- higher the concentration = more efficient but more damage to peritoneal membrane i.e. short life of PD > HD
- HCO3 better than lactate
Chronic:
compensation
increased excretion per functional nephron
reduced tubular resorption
PTH high in chronic
Low Ca
High PO4
reduced growth
anaemia
osteopenia
small kidneys on US (v large in acute)
if minimal haematuria / proteinuria
Acute ? Tubular interstitial nephritis (ibuprofen, antibiotics)
Chronic tubulointerstitial nephritis:
- Nephronophthisis / medullary cystic kidney disease complex (MCKD)
- Nephronopthisis (AR) > ESRF <20yo
- Autosomal dominant tubulointerstitial kidney disease (ADTKD) > ESFR 20-70yo
- Uromodulin kidney disease (UKD) – mutations in the UMOD gene encoding uromodulin (prev MCKD2)
- associated with precocious gout (hyperuricaemia)
- ADTKD due to REN mutations (ADTKD-REN) – mutations in the REN gene (prev familial juvenile hyperuricemic nephropathy type 2)
- associated with precocious gout, anemia, hypotension, or hyperkalemia
- Mucin-1 kidney disease (MKD) – mutations in the MUC1 gene (prev MCKD1)
- Uromodulin kidney disease (UKD) – mutations in the UMOD gene encoding uromodulin (prev MCKD2)
- Lead nephropathy (interstitial)
Note of cystic Kidney disease (ARPKD, ADPKD, NPHP, ADTKD)
- thought related to cilia (?chemosensory role) present on all renal epithelial cells
- see below figure
Acute Renal Failure/Insufficiency = pRIFLE
Kidney Disease Improving Global Outcomes (KDIGO) acute kidney injury
- Stage 1: UO <0.5ml/kg/hr for 6-12h OR Cr increase 150-200% OR CR increase >27umol/L
- Stage 2: UO <0.5ml/kg/hr for >12h OR Cr increase 200-300%
- Stage 3: UO <0.3 mL/kg/hr for ≥24 h, OR Anuria for ≥12 h OR Cr increase >300% OR Cr >350 OR eGFR <35
Chronic Kidney Disease = GFR <60ml/min/1.73m2 for >3m
- stage 1: >90
- stage 2: 60-89 (mild)
- stage 3: 30-59 (mod) (a=30-44, b=45-59)
- stage 4: 15-29 (sev)
- Stage 5 aka failure: <15 or on dialysis
End-stage Renal Disease = those on renal replacement therapy i.e. dialysis or transplanted
Slowing progression
- Strict BP control shown to slow progression
- ACEi and ATIIRB reduced BP and proteinuria
- Low protein diet not show to reduced progression in children
- Treating anaemia not shown to reduced progression but aids growth
Complications
Hyperkalemia
- low K diet
- frusemide
- RRT
- Primarily EPO deficiency
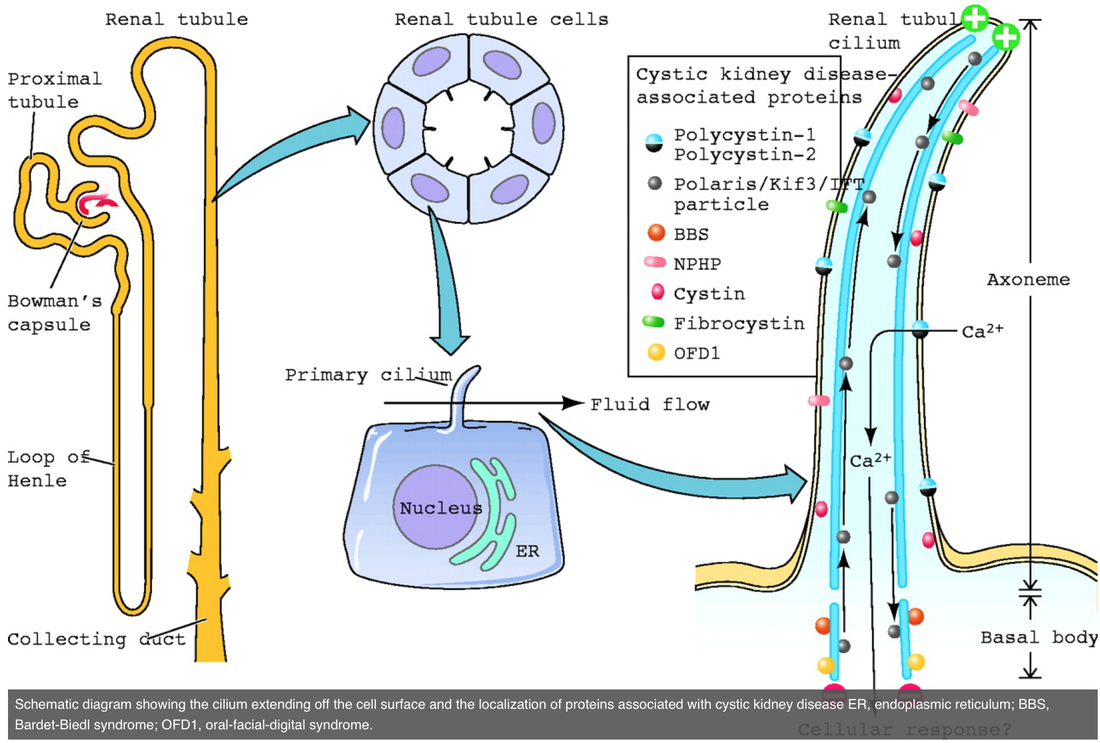
Cystic Kidney Diseases: All Roads Lead to the Cilium
Qihong Zhang, Patrick D. Taulman, Bradley K. Yoder
Physiology Published 22 July 2004 Vol. 19 no. 4, 225-230